
Eczema describes a set of inflammatory skin disorders characterised by dry, red, itchy skin. It presents on different body sites depending on the cause and is one of the most common skin conditions, affecting 1 in every 12 adults (All Party Parliamentary Group on Skin, 2003; National Eczema Society, 2010). Eczema is a highly individual and variable condition, often presenting in the long term, although it can exhibit acute episodes as well. Since it is a challenge to self manage, nurses, particularly those working in the community setting, must be confident in knowing how to support patients. This may be by accessing appropriate information, providing choices of emollient products to use, optimising topical therapies, providing medical advice and signposting patients when needed.
This article outlines the different presentations of eczema in adulthood and how to recognise and treat them. For community prescribers, it is important that they are knowledgeable about local formularies and the first-line therapies available, as well as when it is appropriate to suggest over-the-counter products.
Definition of eczema
Eczema can be classified as endogenous, exogenous or having no known cause (Ashton et al, 2005). Endogenous eczema develops as a result of internal factors that compromise the skin's integrity, for example, atopy (a predisposition to allergic conditions such as asthma, hayfever and eczema), or venous hypertension/varicose veins leading to eczema on the lower legs.
Exogenous eczema develops as a result of contact with external agents in the person's environment that irritate the skin, such as chemicals, fragrances, metals and dyes. Unclassified eczema presents when there is no clear endogenous or exogenous cause.
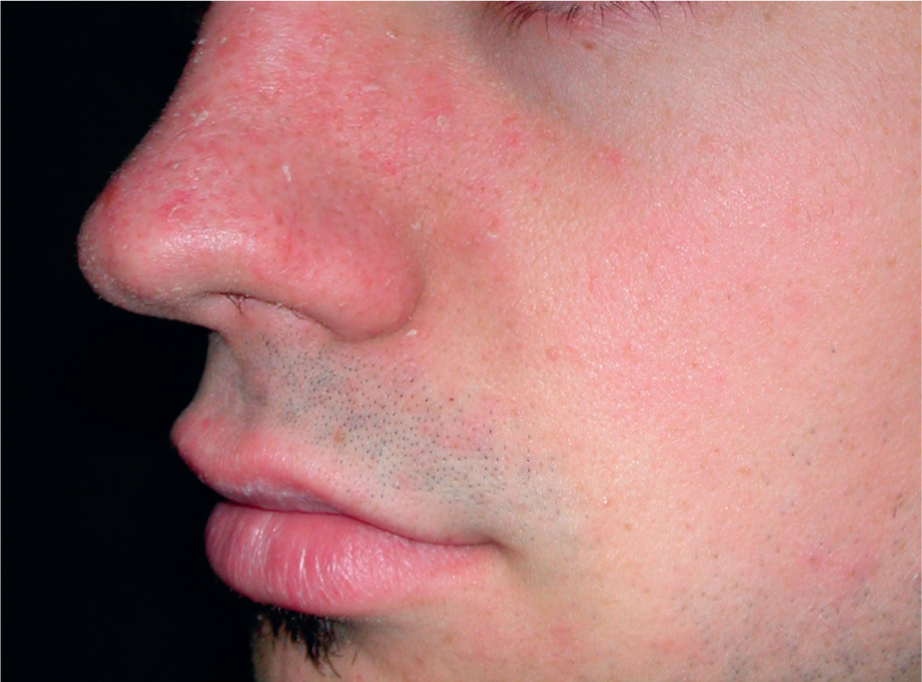
Regardless of the cause, the symptoms of eczema are the same, although they could be widespread or localised depending on the cause (Figures 1–6).





Diagnostic features and types of eczema
Although eczema presents several characteristics that are useful for diagnosis, some of these are non-specific, so the features must be assessed holistically for accurate diagnosis. The main diagnostic features of eczema include pruritus or itching; eczematous eruption with inflammation, redness and possibly vesicles (small blisters); dryness and scaling; a tendency towards ‘sensitive’ skin; a personal history of asthma or allergic rhinitis and childhood onset of eczema (Walling and Swick, 2010).
Adults can experience various forms of eczema:
Assessment
A holistic assessment to determine the cause of eczema should include the following:
Treatment for eczema
The aim of treating any form of eczema is three pronged: to repair and maintain good skin integrity, alleviate symptoms and improve quality of life. Older people may need more time and explanations in order to understand the condition and the therapies suggested. Within a community setting, the mainstay of treatments for eczema are topical. Table 1 provides a review of treatments that can be used within primary and community care settings.
| Lifestyle interventions | Avoidance of soap-based products, i.e. shower gel, bubble bath, soap, shampoo, Dettol |
| Bathing technique—discuss use of soap substitutes or bath mats | |
| Humidification of environment, not too hot or dry | |
| Avoidance of exacerbants or irritants if known, e.g. soaps and fragrances | |
| Wash hair separately from body to avoid shampoo suds on the skin | |
| Avoid animal dander or damp dust when cleaning to avoid releasing dust | |
| Topical therapy | Emollients or moisturisers to be used as soap substitutes as well as leave-on applications to soak into the skin to rehydrate or provide occlusion. See local formulary or Medicines Complete (Royal Pharmaceutical Society, 2019) for products. These include creams, gels, sprays and ointments |
| Application of all topical treatments in line with hair growth to avoid folliculitis, i.e. downward strokes | |
| Antibacterial emollient washes for those with broken skin at risk of infection | |
| Appropriate leave-on emollient—level of greasiness depends on how dry the skin is, e.g. cream or gel/ointment | |
| Discuss fire hazard with the use of paraffin- and non-paraffin-based emollients (Ersser et al, 2007; Medicines and Healthcare Products Regulatory Agency, 2019) | |
| Topical corticosteroids (first line)—when eczema is inflamed, red, irritated and itchy. Four strengths of steroids—mild, moderate, potent and very potent | |
| Potency depends on body site and severity of eczema, e.g. facial or genital eczema requires mild/moderate potency, whereas the palms or soles may need very potent. Discuss this with the prescriber | |
| Finger tip units (FTU) are a guide to the amount to use, e.g. one finger tip full of steroid, from the finger tip to first crease of finger/1/3 finger, is enough to cover the amount of eczema measured by two flat palms. An adult may need up to 7 FTUs to cover their trunk if extensive (Long and Finlay, 1991) | |
| Aim for period to settle eczema and then step down frequency, e.g. daily for 7 days, then 3x a week, 2x week then stop (MeReC, 1999; NICE 2018) | |
| Anti-yeast ingredients needed in combination with steroid for seborrhoeic eczema | |
| Management of venous hypertension with compression in addition to topical therapies for varicose eczema | |
| Topical calcineurin inhibitors (second-line therapy when steroids are ineffective, with advise from dermatology specialist practitioner), e.g. tacrolimus and pimecrolimus |
Referral to secondary care
Not all red and itchy skin is eczema. If more than one person within a residential setting has symptoms, then it is important to consider scabies. Other itchy skin conditions include urticaria, blistering or bullous disorders (pre-blistering) and fungal infections. Some systemic conditions also present with itchy skin, but without a rash, such as diabetes, renal or liver failure, hyperthyroidism, anaemia and leukaemia. If in doubt, a dermatological opinion should be sought, which will usually be in a secondary care setting.
Conclusion
Eczema is a common skin condition in adults and may impair quality of life and lead to breakdown of skin integrity if not identified and managed. Community nurses are well placed to examine patients' skin and recognise dry skin, a precursor to an eczematous response, as well as identify eczema itself. Referring to local formularies will enable staff to appropriately manage eczema with emollients and topical steroids. Staff can supplement their knowledge by referring to material from the National Eczema Society (2010) as well as other reputable dermatology sources.