

Astoma is a surgically created opening in the abdomen that allows for the diversion of faeces or urine outside the body (Marinova et al, 2021). There are three main types of stomas: ileostomy, colostomy, and urostomy, which can be temporary or permanent.
Stoma patients require continuous support throughout their entire life with a stoma, and this often is done through established stoma patient pathways (Davenport, 2014; Marinova and Marinova, 2023). Although stoma patient perioperative pathways exist, these are normally not universal across the UK or the world. Furthermore, patients may not be fully prepared to manage their specific stoma type, especially in the first few months postoperatively, and it may be challenging to achieve independence/self-care while still in hospital, as each stoma – for example, ileostomy, colostomy, urostomy – requires tailored advice and care. If patients do not fully grasp the provided education and advice in the immediate pre- and postoperative period, this may lead to some stoma patients struggling after discharge. If patients’ stoma-specific needs are not addressed, this may lead to avoidable complications and, in some cases, even hospital admissions. Therefore, it is becoming increasingly necessary to develop stoma patient pathways tailored to different patient groups, rather than manage everyone under the same standardised pathways, which is in line with many other personalised stratified follow-up pathways (Røsstad et al, 2013; NHS England and NHS Improvement, 2020).
Therefore, this article explores in detail the ileostomy patient-specific domain that healthcare professionals must be educated on, to ensure patient care is delivered appropriately. Follow-up articles will explore the colostomy and urostomy personalised stratified follow-up pathways.
An ileostomy is created from the lower part of the small intestine, known as the ileum. Because the large intestine is no longer part of the digestion process, water, salt and nutrients that would normally be absorbed there, are lost through the ileostomy. Bile and pancreatic juices are secreted into the small intestine to assist with digestion, resulting in the output from an ileostomy being consistently semi-liquid (porridge-like) or liquid in nature (Marinova et al, 2021).
Approximately one in every 335 people in the UK have a stoma (Colostomy UK, 2022). This equates to approximately 205000 ostomates (Marinova et al, 2021), of which over 100000 have an ileostomy. Roughly 9000 new ileostomies are formed each year in the UK (Fellows, 2017; Lister et al, 2020).
Evidence suggests that patients with an ileostomy are more likely to experience peristomal skin complications, which are usually also more severe than other types of stomas (Taneja et al, 2017; Salvadalena et al, 2020). Additionally, patients with an ileostomy are more likely to experience postoperative hospital readmissions due to dehydration and in some cases, kidney injury (Messaris et al, 2012; Paquette et al, 2013; Liu et al, 2021).
To ensure that ileostomy patients are well-supported after discharge and to prevent unnecessary hospital admissions or appointments with clinicians, ileostomy patients need quick access to specialist services, run by stoma specialist nurses (RCN, 2009; Davenport, 2014; Carter, 2020). Many stoma care services have advice lines, that respond promptly, ensuring patients are supported in a timely manner. However, these are not available 24 hours a day and are often only open on weekdays and between 9am to 5pm, leaving patients without specialist support out of hours. Therefore, it is important to provide education to both patients and healthcare professionals in the community, so they have the required knowledge to manage ileostomy complications.
Guided by these objectives, the author's stoma care department has implemented strategies to prepare patients for a life with an ileostomy, aiming to reduce complications, as well as hospital readmissions, by educating both patients and healthcare professionals.
The author's stoma care department provides all their patients with a Stoma Care – A Guide for Patients book (Figure 1), where all the relevant information regarding diet, hydration, complications management and lifestyle advice is provided before surgery. The book is especially useful once patients are discharged back home, ensuring that all the information is stored in one place and easily accessible, avoiding multiple leaflets, which often get lost (Marinova et al, 2021). The patients are shown which sections are relevant to them – for example, ileostomy – to ensure that they understand the advice which is tailored to their specific needs.
In addition, to ensure a smooth transition from secondary care to community and primary care, general practitioners and community services must be supported too, so that they are equipped with the required knowledge to recognise the specific needs of individual stoma patients.
Diet with an ileostomy
An ileostomy is a life-changing surgery, performed to save or improve patients’ lives. As such, lifestyle adjustments are essential to ensure that these patients adapt to the physiological changes in their lives. Maladjustments to diet and hydration are some of the most common reasons for complications in ileostomy patients, including dehydration, obstruction, stoma appliance leakages and vitamin and/or mineral deficiencies (Marinova et al, 2021; Burch, 2022).
As part of ileostomy patient personalised stratified follow-up pathways, patients must be educated to avoid certain foods, such as high-fibre, spicy foods and deep-fried foods, in the immediate postoperative period and up to 6 weeks after their ileostomy-forming surgery. This is to ensure that common complications such as high output and stoma obstruction are avoided (Burch and Black, 2017; Marinova et al, 2021). See Table 1 for a list of foods patients are advised to include or avoid after ileostomy surgery.
| Foods to include | Foods to exclude | ||
|---|---|---|---|
|
|
|
|
|
As an average, ileostomy output is 600–800ml/24 hours. Loss of minerals such as salt is expected, and therefore patients should be advised to add more salt to their diet, if appropriate.
Patients should also be taught to initially measure their stoma output and adjust their diet and hydration, as well as titrate antidiarrhoeal medications according to ileostomy output.
Ileostomy patients are usually educated to follow this type of diet as part of preoperative counselling and postoperative care, but many patients in general forget or have minimal recollection of all the provided medical information once discharged home (Kessels, 2003). Therefore, it is very important that healthcare professionals who may be looking after these patients are also aware of their specific dietary needs so that they can reiterate the diet advice if needed.
Patients and healthcare professionals should also know that avoiding these foods is generally advised in the immediate 4–6 weeks after surgery, and these should slowly be reintroduced after the initial few weeks of postoperative recovery. It is important to note that most patients with an ileostomy should be able to return to eating most foods after the first 1–2 months of recovery and bowel adaptation, or at least have these foods in moderation, as their consumption may increase their ileostomy output, and in some cases, if not cooked or chewed well, may cause blockages. Nevertheless, when patients are unwell, whether it is due to cold/flu, intestinal blockages or anything else, these events may worsen ileostomy function and patients may need to temporarily revert to more bland, low fibre, non-deep fried and non-spicy foods while recovering. However, patients must always be considered as individuals, and be made aware that different foods may have different impacts on their ileostomy.
Hydration with ileostomy
Another important part of personalised, stratified follow-up pathways for ileostomy patients is ensuring that they have good knowledge of hydration. Being well-hydrated and knowing which fluids to drink is essential. Patients with ileostomy, as well as healthcare professionals, must be welleducated and know how an ileostomy reacts to different drinks, as non-adherence to such advice may lead to increased or high stoma output, dehydration, and in some cases, to kidney injury and hospitalisation. Table 2 demonstrates examples of fluids patient should avoid or include to ensure their ileostomy output is within normal range.
| Drinks to include | Drinks to exclude |
|---|---|
|
|
|
Fluids such as rehydration solutions (Dioralyte™ and St Mark's E–Mix, WHO oral rehydration solution) and drinks rich in salt (vegetable/meat stock, Oxo®, Bovril®, Knorr®) have ideal concentrations of salt, which helps ileostomy patients' body achieve balance and stay hydrated. This is especially important in the immediate postoperative period, as well as whenever these patients may be at risk of dehydration – hot weather or vigorous exercise with excessive sweating, vomiting, and increased stoma output (Marinova et al, 2021). To ensure patients are empowered to manage their condition independently, as part of patient-centred follow-up pathways, they should be educated and prepared for occurrences when dehydration may occur, so that they can prevent and/or treat it promptly. If they are struggling to manage this independently, then their family, carers, and other healthcare professionals responsible for their health, must also be educated to support them.
When these episodes occur, patients and healthcare professionals must remember that it is essential to understand that when an ileostomy patient experiences high stoma output (>1200–1500ml), they should never be advised to have plenty of fluids. Instead, they should be advised to add more salt to their diet, have isotonic drinks, such as St Mark's E-mix solution, or other similar oral rehydration solution, limit irritant drinks and limit fluids to 1.5 litre/24 hours, because excessive intake of hypo-/hypertonic fluids further stimulates the intestine leading to excessive stoma output and worsening of high output, potentially leading to dehydration (Nightingale, 2021). The more hypotonic (eg tea, coffee,‘diet’ drinks, water and squash) and hypertonic fluids (eg juice, alcohol, energy drinks, fizzy drinks and Ensure® drinks)that patients drink when their stoma is of high output, the more dehydrated they get and the thirstier they feel, as part of osmosis. Such fluids result in the intestine producing increased bowel effluent, leading to worse symptoms of potential dehydration. Therefore, they must have isotonic drinks instead to ensure appropriate hydration and stop the vicious cycle of drinking plenty of hypo-/hypertonic fluids, which then worsens their high output stoma symptoms.
Medications
Another important element of ileostomy patients-centred follow-up pathways is ensuring that these patients have a good understanding of medication management specific to their condition.
Foremost, they may require medications to manage their stoma output, to prevent dehydration when the stoma output is of high volume. To manage this, patients are usually advised to use antimotility or antidiarrheal medications, as they slow down intestinal peristalsis, allowing fluids and nutrients to be better absorbed by the intestine. Therefore, these medications are generally administered at least 30minutes before meals, with a small amount of water (Marinova et al, 2021; Nightingale, 2021).
Below is a list of the most common medications used to manage increased/high output stoma:
Additionally, people with an ileostomy are more likely to have problems with malabsorption of medications, especially if they have high output. Therefore, modifiedrelease medications should be taken with caution. However, patients and healthcare professionals must be also educated about the ‘ghost tablets phenomenon’ (Tungaraza et al, 2013). Sometimes patients may pass what appears to be undigested tablets or capsules in their stoma bag. Usually, this is just the shell or protective covering which holds the drug, as the actual active ingredient of the medication has already been absorbed by their body. This phenomenon is known as ‘ghost pills’ or ‘ghost tablets’ and is common with many modified-release medications. However, in people with a high output ileostomy or jejunostomy, the medication may not be absorbed. If there are concerns that the patient is not getting the benefits of their medication they must discuss this with their GP and discuss the need for different forms of medication (Marinova et al, 2021).
There are also recommendations that certain medications may need to be avoided and/or temporarily stopped when ileostomy patients have very high output, to ensure kidney injury is avoided. These recommendations are also known as ‘sick day’ guidance for patients at risk of acute kidney injury. These include temporary discontinuation of antihypertensive, diuretics, some heart medications, NSAIDS and diabetic medications (Martindale et al, 2017). Patients must be assessed to ensure benefits outweigh the risks.
Similarly, patients with ileostomy must be advised not to take laxatives as these may cause severe dehydration and kidney injury.
Lastly, it is essential to educate patients and healthcare professionals that due to risks of malabsorption in acute episodes, with increased stoma output, other medications, such as contraceptives, may need to be reviewed, as they may not be as effective due to the potential decreased absorption. Alternative options such as patches may be more appropriate (Moore, 2015).
Routine tests
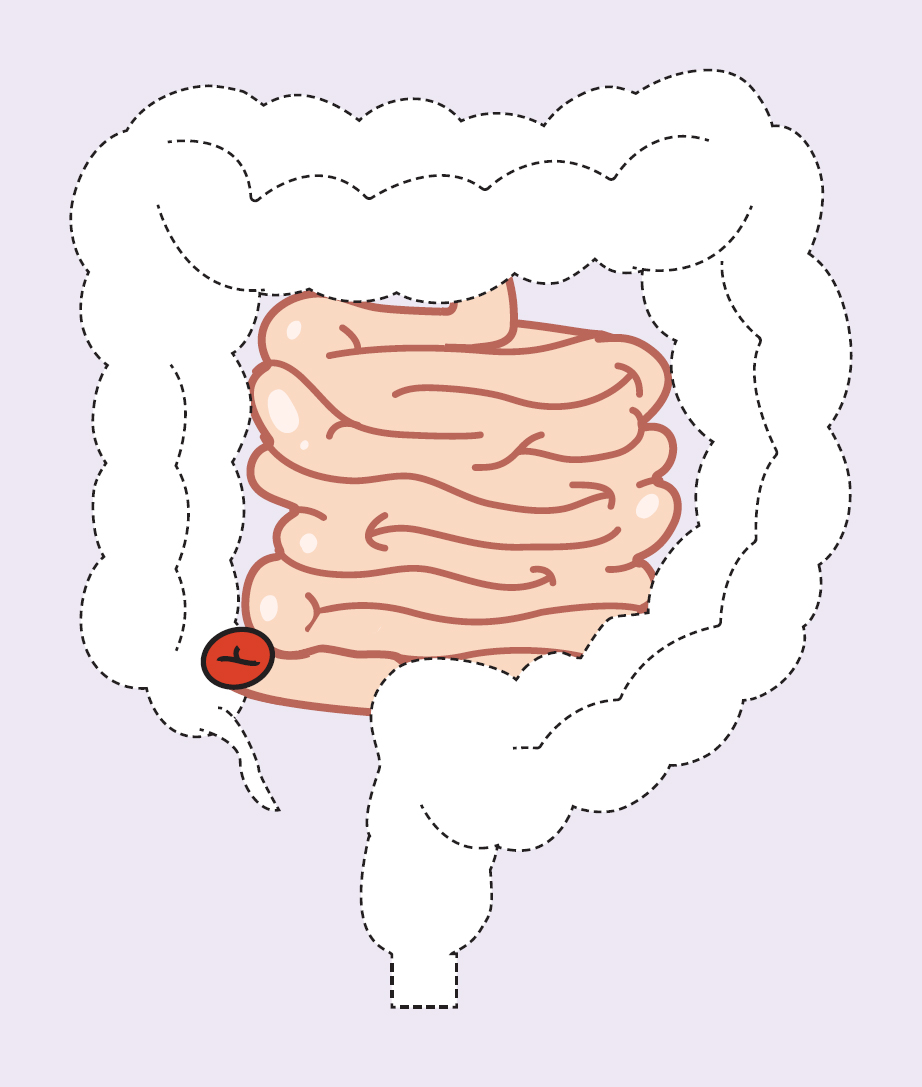
Patients with an ileostomy are more prone to vitamin and mineral losses, since a significant part of their bowel (colon) is not functioning anymore or is removed. Furthermore, the end section of their small intestine – the ileum – may be removed or used to form an ileostomy (Figure 2) (Nightingale, 2021). Therefore, as part of best practice for these patients’ care, it would be recommended to have routine annual blood tests such as liver function tests, urea and electrolytes, calcium, ferritin, folate, vitamin D and vitamin B12, along with random urine sodium, when dehydration and malabsorption may be suspected or if the patient is considered at higher risk (Nightingale, 2021; Michońska et al, 2023). These are the standards at the authors’ stoma care department. These routine tests are normally requested by the patient's GP to ensure any deficiencies are caught on time and treated accordingly. Nevertheless, patients and healthcare professionals must be educated that the risk of vitamin and mineral deficiency is not associated with having an ileostomy per se; it is due to the colon, and sometimes part of the small intestine, having been removed or not being in continuity, whether this is a temporary or permanent stoma (Severijnen et al, 2004).
Stoma appliances and accessories
A lot of areas and NHS organisations promote the use of formularies and prescription guidelines for stoma care products, and the general advice for the use of appliances in ileostomy patients is 10–30 stoma bags a month, taking into consideration the frequency of stoma bag changes, which generally is once every 1–3 days (PrescQIPP, 2015). However, patients with newly formed stomas, as well as patients with problematic stomas, may be using more products, and therefore, regular stoma nurse appliance and prescription reviews are advised at least 4–5 times in the first 6 months, and then once a year or more often if any concerns are present. This is to ensure patients are well-supported, and waste is limited, where possible. Hence, patient-centred pathways are essential to ensure that their specific needs are taken into consideration and their care is not compromised.
Ileostomy patients are more prone to experiencing leakages, more severe peristomal skin complications leading to a substantial impact on the quality of life of these patients, as well as increased costs as a result of managing complications (Rolls et al, 2023).Therefore, it may be advisable to consider use of convex stoma bag appliances as first choice to minimise the risk of leakages and associated complications, because use of convex bags is known to minimise the incidence of leakages (González et al, 2021).
Additional products such as stoma paste, seals and flange extenders are known as accessories. These are not routinely prescribed and are usually reserved for those patients suffering from complications. However, the use of accessories will also depend on patient-specific needs, including the type of stoma (PrescQIPP, 2015; Marinova et al, 2021).
When it comes to ostomates, it is imperative to highlight that one stoma bag or brand does not fit all, and therefore, it is not appropriate to recommend a generic brand for all patients when using formularies. Stoma bags are also skin care products and stoma nurse specialists choose one based on their patient-specific needs. This concept is similar to other health conditions (for example, epilepsy, Parkinson's disease) where specific medication brands must always be used to ensure the best results.
Furthermore, while formularies and guidelines normally suggest recommended guides on the use of a certain amount of products per month/year, this would also depend on many factors and clinicians should consider that sometimes a formulary recommendation and prescription guidelines may not be appropriate for all patients, especially those with complex stoma needs.
Therefore, all these factors must be considered whenever healthcare professionals make prescribing decisions for these groups of patients.
Patient follow-up
Though ostomate follow-up pathways vary in different areas, many of them adhere to a similar approach, where primary importance is given to the initial 3 months post-operatively, while patients are still adapting to life with a stoma.Therefore, more frequent follow-ups are provided in these initial 3 months. The authors' tertiary hospital relies on a structured follow-up, and local patients are offered intensified follow-ups in the initial 30 days postoperatively – clinical review every 10–14 days or more often, if complications occur. This then reduces in frequency and patients are seen at month 3, month 6 and month 12, and then moved to an annual follow-up (Marinova and Marinova, 2023). Although a structured pathway is being used, these are not tailored to different stoma types and do not make recommendations based on different patient groups. Whether patients are seen more often, will also depend on how well they are adapting to their ileostomy, or whether they have any complications. Ileostomy patients have the highest complication rate in comparison to colostomy and urostomy patients (Ma et al, 2022). These patients are also more likely to experience stoma appliance leakage (González et al, 2021).Therefore, it should be anticipated that they may be more likely to require additional reviews by stoma nurse specialists; they may not necessarily fit into the established pathways, as they may require additional appointments, whether planned or ad hoc, as well as access to remote/digital advice lines.
Patients with ileostomies have a higher rate of hospital readmissions. Schott et al (2022) found that within 120 days of discharge, 52.3% of patients with ileostomies were readmitted, compared to 36.3% for colostomies and 34.6% for urostomies. Often, especially in the period immediately after discharge with a new ileostomy, these patients' complications may cause great distress and ineffective coping mechanisms, which may result in them seeking immediate help rather than trying to resolve the problem at home. In similar cases, home telephone support, as well as access to an advice line and patient care handbook, have proved to be essential in reducing these incidents in the authors' settings.
Therefore, it is important when planning workforces and workloads, to always consider that ileostomy patients are more likely to require an increased number of reviews, which must be carefully planned into annual workforce planning.
Important considerations
Ileostomy patients require support throughout their entire journey with a stoma. Given the fact that they are more likely to encounter complications, it is of paramount importance that stoma care services are available for them to ensure continuous support, but other healthcare professionals are also equipped to provide support in all settings of healthcare. Providing this support requires investment in the NHS workforce, infrastructure and standardised patient pathways, to ensure that patient care is similar, regardless of the area they live in. Ensuring there are enough stoma specialist nurses is crucial for providing optimal care to stoma patients. These nurses play a vital role in reducing costs, alleviating pressure on emergency departments, and easing the burden on general practitioners and consultant clinics by independently managing stoma patients in nurse-led services.
Conclusions
Creating well-defined pathways that guide patients and healthcare professionals through the perioperative journey of stoma-forming surgery is crucial for ensuring excellent patient care and positive outcomes. These pathways should also be tailored to match different patients and types of stomas’ unique needs, as this will allow for a more patient-centred care and improve patients’ outcomes. To achieve this, stoma care services must have adequate resources to provide uninterrupted care throughout an ostomate's entire journey.
Additionally, healthcare professionals in all settings of healthcare – primary, secondary and community settings – should be equipped with the necessary knowledge to provide care for these patients and help reduce complications and hospital admissions.